Mechanical CPR: not all it's cracked up to be
Why does mechanical CPR have WORSE outcomes that human compressions?

Anyone who’s done CPR knows that it can be exhausting, especially if you are doing it for many cycles. As your arms tire, the compression depth decreases, the rate slows, and the quality drops. Evidence suggests that the quality of CPR drops rapidly with fatigue and poor-quality CPR means poor outcomes.
So why not automate it?
Robots are well suited for repetitive mechanical tasks, able to perform the identical motion with perfect tempo. It’s a compelling idea. Currently available devices include the Lund University Cardiopulmonary Assist System (LUCAS, Stryker Medical), the AutoPulse (ZOLL Medical Corporation), and the Thumper (Michigan Instruments). And yet, despite decades of development and clinical use, mechanical CPR devices haven’t improved outcomes in any clinical trial.

Not only that, 6 observational studies and 2 RCTs have found worse neurological outcomes with mechanical CPR:
The observational evidence is consistent and damning. The largest comes from the CARES national registry: Buckler and Rossano analyzed over 80,000 cardiac arrests and found that mechanical CPR was associated with lower neurologically favorable survival and strikingly, EMS agencies that never used mechanical CPR at all had the best outcomes. Liao et al reached similar conclusions using the Utah CARES registry, finding a relative risk of just 0.41 for functional survival after propensity-score adjustment in patients receiving mechanical CPR. Hayashida et al prospectively followed over 6,500 patients across 67 Japanese hospitals and found that mechanical CPR in the emergency department was independently associated with lower ROSC, lower hospital admission rates, and lower survival to discharge. Putzer et al found a 30-day survival rate of just 5.1% with LUCAS versus 16.3% with manual CPR in an unselected Austrian OHCA population. Kim et al, drawing on a nationwide South Korean registry of over 20,000 patients, found that every mechanical device tested was associated with lower ROSC, with AutoPulse specifically linked to significantly worse survival to discharge.
It’s tempting to attribute these findings to confounding: perhaps sicker patients or longer codes are selectively getting the machine? But the randomized data tells the same story. The ASPIRE trial was stopped early after mechanical CPR patients had nearly half the survival to discharge of manual CPR patients (5.8% vs 9.9%). PARAMEDIC, the largest RCT, found no improvement in 30-day survival and lower rates of favorable neurological outcome at 3 months. Among survivors who were followed long-term, MMSE scores were modestly but significantly lower in the LUCAS group, a signal that even patients who survived may have paid a cognitive price for mechanical CPR.
We should also consider the counterfactual. If mechanical CPR was really better, wouldn’t we expect to see improved outcomes with it somewhere? And yet, despite decades of use and dozens of studies - both randomized and observational - none has demonstrated a compelling benefit to mechanical CPR.
So why doesn’t the tireless machine achieve better outcomes than the fallible, fatiguable human?
Interruptions Kill
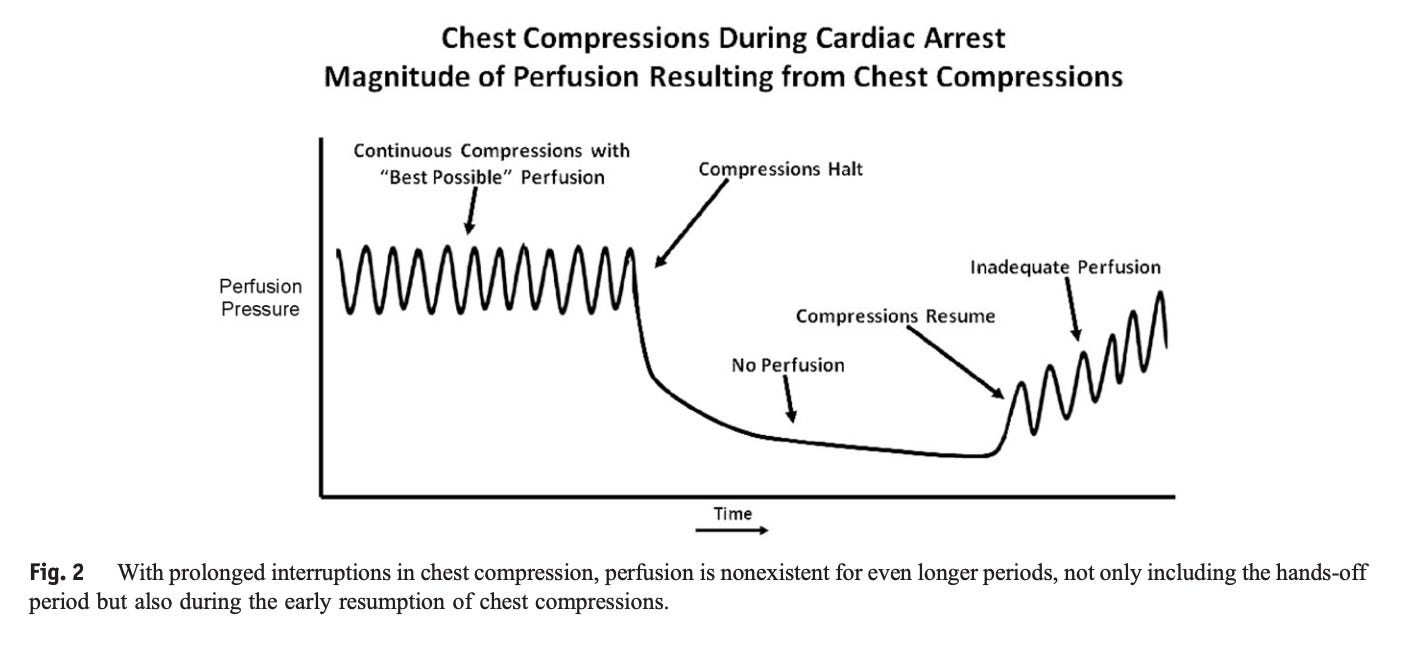
Even brief interruptions in compressions markedly reduce coronary perfusion pressure. Edelson et al. found that a 10-second interruption of CPR prior to defibrillation reduces the rate of ROSC by almost 50%. (This is why charging the defibrillator before the rhythm check matters so much - you minimize the pause between “stop compressions” and “shock.”) Every second of no-flow time is a second the brain isn’t being perfused, and it takes time to restore perfusion pressure after each interruption.
Putting on a mechanical CPR device takes time - time during which no compressions are being delivered.
A 2007 study found that the mean time to set up the AutoPulse™ was 4.7 minutes, though it’s unclear how long compressions were stopped for. A 2012 study by Yost et al. found that compressions were paused a median of 32.5 seconds (IQR 25–61 seconds) to apply the LUCAS device. That means more than a quarter of patients had no compressions for over a minute while the team strapped on the machine.
Maybe it’s a training problem? Steffen et al. trained medical students to rapidly apply a mechanical CPR device, which reduced the deployment time from a median of 37.0 seconds (IQR: 29.0–42.0) in the control group to 26.0 seconds (IQR: 20.0–30.0) after training. That’s still a long interruption. And in a follow-up assessment four months later, the time had crept back up to 34.5 seconds (IQR: 24.0–45.8), suggesting that the benefit of training is both minimal and transient.
The Machine Isn’t Even Better at the Mechanical Part
Here’s the counterintuitive finding: the machine frequently fails at the one thing it was built to do.
A 2011 manikin study compared conventional versus mechanical CPR as performed by 21 ambulance crews. Only 58% of compressions delivered by the LUCAS device were adequate, compared to 88% with manual CPR. And only 12 of the 21 crews (57%) correctly applied the mandatory stabilization strap.
Why? Mechanical CPR devices frequently become displaced during a resuscitation. A device that has shifted even a few centimeters may be compressing the upper abdomen instead of the sternum. Malpositioned CPR is worse than tired CPR.
There’s also a subtler problem. Human rescuers naturally vary the force they deliver, which allows adequate chest recoil between compressions. Mechanical devices deliver metronomic compression, which sounds like a feature, but may actually impair venous return if there isn’t sufficient recoil time. The heart needs to refill between compressions; if it can’t, cardiac output drops regardless of how fast or consistently you’re pushing.
This was demonstrated in a pediatric cardiac arrest study that randomized piglets to either mechanical or conventional CPR. Survival was significantly higher in the conventional CPR group (50% vs. 15%, p = 0.016), suggesting humans may be doing something mechanically beneficial.
Mechanical CPR Causes More Injuries
A meta-analysis of 11 trials found that mechanical CPR was more likely to cause injuries than manual CPR. Rib fractures, sternal fractures, liver lacerations, and in the case of a displaced device, injury to abdominal organs. I’ve personally seen this: a malpositioned mechanical CPR device doing vigorous, regular compressions directly over a pâtéd liver.
Beyond displacement and injury, there’s the specter of device failure itself. A 2025 study examined 255 failures of the LUCAS device reported to the FDA. These included fractures, soft tissue injuries, and injury to internal organs. Device failures occurred in 54% of reports, in many cases leading to prolonged interruptions in CPR. This is a failure mode totally unique to mechanical CPR; even tired humans don’t suddenly freeze and prevent compressions from being performed.
Where Mechanical CPR Does Make Sense
There is a role for mechanical CPR. There are situations where human CPR cannot be safely or practically delivered: on a sled coming off a ski slope, in a helicopter, or under fluoroscopy in the cath lab. In those austere or logistically constrained settings, an imperfect device beats no compressions at all.
The key word is substitute, not supplement. Mechanical CPR should be used where humans cannot do the job, not as a default upgrade over humans who can.
Are These Machines Worth the Cost?
The LUCAS 3 costs approximately $15,000 per unit. Add training, maintenance, and replacement parts, and the total cost of ownership is substantially higher. Most EMS systems have multiple units across multiple vehicles.
Now ask a different question: how much community CPR training could be purchased for the same investment? Bystander CPR performed by imperfect, sweaty humans demonstrably saves lives: It roughly doubles survival rates from out-of-hospital cardiac arrest. Training programs cost on the order of $30–50 per person.
Every dollar spent on a device that demonstrably doesn’t improve outcomes is a dollar not spent on community CPR training, which does.

Amazing work, thanks!